Synthetic materials for managing POP and urinary incontinence
Article authors


 |
Prof. Dmitry Pushkar Urology Department Moscow State Medico Stomatological University Moscow (RU) |
 |
Dr. George Kasyan Urology Department Moscow State University of Medicine and Dentistry Moscow (RU) |
We live in an era in which synthetic materials are used extensively in medicine. Pelvic organ prolapse (POP) repair and the treatment of stress urinary incontinence using traditional surgical techniques is associated with a high rate of recurrence 1.
Currently, synthetic tapes and meshes are frequently used in these types of surgery with very good clinical outcomes 2 . At the same time, there has been an increase in the number of mesh-associated complications. Although rare, these complications can have serious consequences.
During the past several years, many reports of complications associated with synthetic meshes have been published in the literature. The most frequent complications include vaginal erosion, mesh shrinkage, infections, pain, urinary tract disorders and a recurrence of prolapse. There have also been reports of rare complications, such as bowel, bladder, and blood vessel perforation during insertion.
In 2011, the joint committee of the ICS-IUGA published a standardised terminology and classification for complications related to synthetic and biological materials in female pelvic floor surgery 3 . This classification is designed to comprehensively cover complications in both insertion and healing. The POP-Q has been used widely around the world for the classification of prolapse and serves as a good example; we hope that this new classifier of prolapse complications will achieve similarly prominent usage.
"Complication is a morbid process or event that occurs during the course of a surgery (or postoperatively) that is not an essential part of that surgery.” -Stedman’s Medical Dictionary
At the same time, there are rare, unique complications that can occur due to the coincidence of multiple uncommon factors. The purpose of this paper is to highlight some of these rare cases and to warn readers of potential problems such as those described here.
Ureteral obstruction
A 23-year-old nulliparous woman was referred by her gynaecologist because of increasing urinary incontinence upon walking and exercising and complaints of urine dribbling or wetness. Uroflowmetry revealed a maximum flow rate of 19 ml per second, and cystometry revealed a stable detrusor. The patient chose to have surgical treatment because she was not benefitting from physiotherapy. She was advised about the possibility of difficulty in delivery after sling surgery.

Figure 1: Right-sided hydronephrosis associated with a dysplastic kidney and an enlarged right ureter draining ectopically into the vagina. (Courtesy of Prof. O. Loran)
In 2005, a transobturator tension-free tape procedure was performed uneventfully. On the first postoperative day, the patient developed right flank pain with no decrease in urine output. Examination revealed tenderness over the right renal angle. Ultrasound examination showed right-sided hydronephrosis. Intravenous urography confirmed right-sided hydronephrosis associated with a dysplastic kidney and showed an enlarged right ureter draining ectopically into the vagina (Figure 1).

Figure 2: Ureteral orifice ectopy into the vagina. (Courtesy of Prof. O. Loran)
Surgical exploration confirmed complete ureteral obstruction at the level of the tension-free vaginal tape (Figure 2). The patient underwent nephroureterectomy with full symptomatic resolution.
Urinary incontinence in young girls who have been toilet trained may be due to ectopic ureter insertion below the urinary sphincter. This diagnosis is frequently delayed until adolescence, it is psychologically distressing, and it may be missed at physical examination. According to the current literature, renal duplication with associated complete ureteral duplication can cause continuous incontinence in young women if the ureter draining the upper pole moiety inserts ectopically below the external urethral sphincter4,5 . Ideally, the diagnosis of this condition should be made in early childhood.
In this case, an unrecognised ectopic dysplastic kidney mimicked stress urinary incontinence, which led to the insertion of tension-free vaginal tape via a transobturator approach; the synthetic tape then caused an obstruction of the vaginal ureter. This case demonstrates that a thorough and attentive approach is mandatory in order to ensure the identification of congenital abnormalities prior to surgery.
Ureteral trauma
A 70-year-old woman with stage III cystocele was admitted to our urogynecological clinic for pelvic organ prolapse (POP) mesh surgery. Anterior transvaginal mesh implantation of a four-armed anterior implant inserted using four trocars passed through the obturator foramen was performed. At the second day post-surgery, the patient noted moderate edema and pain in her right hip. Her temperature was 37.2 ºC, and the blood tests revealed normal white and red blood cell counts. A contrast CT scan showed urinary leakage on the right side (Figure 3A) extending to the interfascial space of the right hip (Figure 3B).
The patient was taken to the operating room. A retroperitoneal approach revealed complete injury of the right ureter at the level of the right posterior arm of the mesh. Ureterocystostomy with Boari flap was performed. Blood loss was minimal, and the operation lasted 75 minutes.
Anatomical landmarks are essential in pelvic organ prolapse repair. During hands-on training for mesh surgeries, it is necessary to pay special attention to safety landmarks and anatomical topography. The ureters are always in close proximity to the cervix, and ureteral injury should be considered as a potential risk in patients with extensive prolapse.
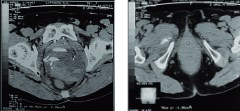
Figure 3: CT scan showing urinary leakage on the right side (A). Urine leakage extending to the interfascial space of the right hip (B).
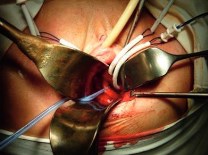
Figure 4: The right ureter is in close proximity to trocars inserted for pelvic organ prolapse repair with synthetic mesh.
Small bowel eventration after POP surgery
A 56-year-old multiparous female was referred to the centre in May of 2008 with the chief complaint of pelvic pain and bladder emptying problems. She had undergone vaginal hysterectomy and the simultaneous insertion of trocar-guided mesh for pelvic organ prolapse (POP) six months prior to referral. Physical examination revealed that the dyspareunia and emptying abnormalities were caused by significant shrinkage of the mesh. She opted for surgical repair and asked that proper sexual function be preserved
After consultation with a pain specialist, a decision was made to proceed with the excision of the vaginal mesh. The folded and shrunken mesh was successfully removed, and the patient was discharged within several days (Figure 5).

Figure 5: The mesh on the anterior vaginal wall is completely shrunken (A). The removal of the mesh (B)
After one month, the patient presented with prolapsed loops of small bowel protruding through the vagina. The event occurred three hours prior to admission. On examination, she was afebrile with stable vital signs, and her abdomen was soft and non-tender. Examination revealed several loops of small bowel protruding from the vagina (Figure 6). The serosal surface appeared pink with visible peristalsis.

Figure 6: Eventration of small bowel through the vagina.
The patient was taken to the operating theatre, where she was prepared and placed in the lithotomy position. The prolapsed small bowel was repositioned after copious irrigation and cleansing. Subsequent investigation revealed a defect on the posterior vaginal wall and peritoneum of the cul-de-sac, which was not properly closed after the previous hysterectomy.
The patient recovered from anaesthesia uneventfully and was discharged the next day. She was re- examined at one month and three months postoperatively, and vaginal cube pessary was used to reposition the vaginal cuff (Figure 7A). A laparoscopic sacrocolpopexy was performed to reduce the prolapse of the vaginal cuff. The postoperative period was uneventful (Figure 7B)

Figure 7: Three months after the surgery (A). The same patient after sacrocolpopexy (B).
Discussion
Modern surgical techniques for the management of stress urinary incontinence and pelvic organ prolapse are presumed to be a minimally invasive with almost no complications. At the same time, it should be emphasised that the implantation of surgical mesh is permanent, that some complications associated with the implanted mesh may require additional surgery, and that even surgery may not correct the complication.
There are some obvious measures that can help reduce the rate of complications. First, each surgeon must obtain specialised training for every mesh placement technique to ensure that he or she is aware of its specific risks. This seems to be particularly important because all synthetic surgical kits are based on different techniques.
Specific risk factors for complications associated with mesh positioning have not been properly determined. Contributing factors may include the overall health of the patient, the mesh material, the size and shape of the mesh pores, the surgical technique itself, the occurrence of simultaneous procedures, such as hysterectomy, and other factors.
Special attention should be paid to complications associated with the trocars for transvaginal placement, especially in the bowel, bladder and blood vessels. However, even close attention to these issues cannot prevent all complications
The European Association of Urology is providing an annual master class on Female and Functional Reconstructive Urology in Berlin to provide a high level training programme for European specialists. Specialised longer-term training for specialists in centres of excellence is an essential and urgent need in EAU postgraduate programs.
References
- Dällenbach P. Incidence and risk factors for reoperation of surgically treated pelvic organ prolapse. Int Urogynecol J Volume 19, Number 12, 1623-1629
- Novara G, Galfano A, Boscolo-Berto R, Secco S, Cavalleri S, Ficarra V, Artibani W. Complication rates of tension-free midurethral slings in the treatment of female stress urinary incontinence: a systematic review and meta- analysis of randomized controlled trials comparing tension-free midurethral tapes to other surgical procedures and different devices. Eur Urol. 2008 Feb;53(2):288-308.
- Haylen BT, Freeman RM, Swift SE, Cosson M, Davila GW, Deprest J, Dwyer PL, Fatton B, Kocjancic E, Lee J, Maher C, Petri E, Rizk DE, Sand PK, Schaer GN, Webb R; An International Urogynecological Association (IUGA)/ International Continence Society (ICS) joint terminology and classification of the complications related directly to the insertion of prostheses (meshes, implants, tapes) and grafts in female pelvic floor surgery. Neurourol Urodyn. 2011 Jan;30(1):2-12.
- Carrico C, Lebowitz RL. Incontinence due to an infrasphincteric ectopic ureter: why the delay in diagnosis and what the radiologist can do about it. Pediatr Radiol. 1998;28:942–949.
- Berrocal T, Lopez-Pereira P, Arjonilla A, Gutierrez J. Anomalies of the distal ureter, bladder, and urethra in children: embryologic, radiologic, and pathologic features. Radiographics. 2002;22:1139–1164